As a child progresses through speech therapy, their speech becomes more intelligible and they become a more competent communicator. There are some speech sounds that seem to be harder for children to acquire (not just those with CAS). These sounds include /r/, /l/, /s/, and /z/. A child with CAS may have acquired motor plans for production of all but 1 or 2 sounds. Usually, their speech is mostly understood by others, but these residual errors are noticeable. A child may not acquire these last sounds until late elementary, middle or high school, or even into young adulthood.
Therapy to acquire these last sounds is similar to their previous therapy. It requires specific remediation which includes many practice trials and can be difficult, leading to frustration, and perhaps the child loses the motivation to continue trying. Other factors for being able to acquire these residual sounds include what sound is in error, any co-occurring disorders, severity of the CAS, and progress made thus far in treatment.
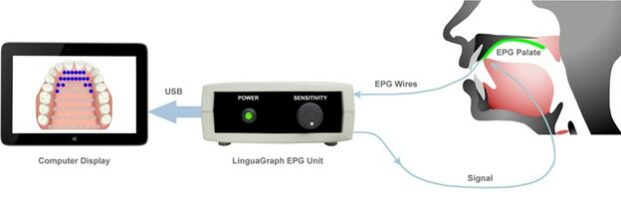
Even though progress is likely to be slow, incorporating different approaches at this stage may be helpful. It is hard to see what the tongue is doing in the mouth when we produce the /r/ sound. There are several types of biofeedback which provides visualization of the speech sound produced, or of tongue movements, in order to produce accurate speech movements.
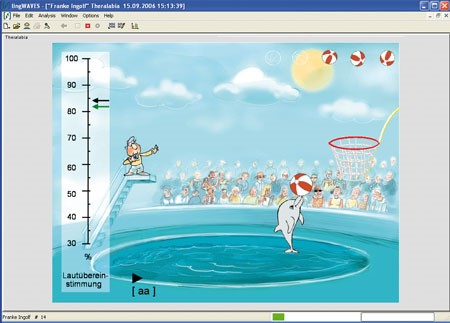
One type is through computer programs or apps that listen to the speech production of a sound the child produces and provide information about how closely the production matches the target (correct) production. The information can be in the form of a game – the correct production by the child will cause the dolphin to put a ball through the hoop. Or the computer can produce visual graphs of how the production matches the target sound. The speech-language therapist (SLP) sits with the child and provides cues to help the child move their tongue correctly in order to produce the sound correctly. The picture below shows the computer screen of the lingWaves program by TheraVox for remediation of speech and voice errors.